A Quick and Comprehensive Approach to the Treatment of Shoulder Problems with Chinese Medicine
Shoulder pain is a common problem for which patients seek relief through Chinese medicine. In terms of its success rate with acupuncture, it is one of the easier musculoskeletal disorders to treat. This article presents four treatment options I commonly choose from for the treatment of shoulder pain, all of which are efficacious and easy to execute. The practitioner is encouraged to review and select those that he prefers upon his predilection that can benefit the patient.
First, regardless of the treatment selected, have the patient explain to you the etiology of the problem; its duration and intensity; what makes it better or worse; and other relevant characteristics. Determine the patient's range of motion by having them move their arm and shoulder in all the normal movements (rotation [lateral and medial]; abduction; adduction; flexion; and extension), and evaluate the patient's type of impaired mobility.
Treatment I: Auricular Medicine
I typically choose ear massage and treatment as my first and only therapeutic modality because of my affinity to auricular medicine and its proven efficaciousness. In the ear, locate the shoulder point if the problem is musculoskeletal or the shoulder joint point if the problem is confined to the joint.
Vigorously rub the chosen ear point between your thumb and index finger. Do this with the patient seated or standing. Let the patient know they will feel a very strong sensation elicited by the rubbing. Perform this step for 15-30 seconds. The stimulus will be very intense, and the patient may grimace or tell you it is painful. After this time span, have the patient perform the shoulder movements that were compromised prior to the massage. In most cases, if your ear point location was accurate, you achieved the desired stimulus (i.e., strong sensation and/or heat), and if the patient could tolerate it, there will be 50-100% improvement in the shoulder. If this technique has been effective but you feel the shoulder needs further reinforcement, you can affix a stainless steel BB or an ear seed to the point so the patient can retain it for about three days. Instruct them to rub the point gently 3-5 times a day for about 3-5 seconds while at the same time mobilizing the affected shoulder.
Figure I: The shoulder and shoulder joint ear points.
If the shoulder problem is along the large intestine channel, select the shoulder point on the contralateral (opposite) side of the patient's shoulder pain. The reason for treating the opposite side is that the large intestine's divergent meridian exits at LI 15 (jianyu). If the pain is more posterior, i.e. along the scalene muscles or in the gall bladder 21 area (jianjing), select the ear point on the same side as the patient's shoulder problem. See Figure I for the location of these points.
Treatment II: Needles
Another interesting treatment of shoulder pain, especially if it appears anterior to the acromioclavicular joint, is to treat the lung. Remember: the lung meridian internally transverses the shoulder area where it exits at LU 1 (zhongfu). With the patient reclining, needle LU 7 (liegue) transversely 0.5-1.0 inches proximally (toward the shoulder). Do this unilaterally on the side of the affected shoulder problem. In this instance, you are using Lung 7 as a longitudinal luo; that is, as a connecting vessel on the lung meridian to send a stimulus to the lung organ/meridian complex. After attaining qi, use a vigorous dispersion technique (I prefer swift speed and a large amplitude) for 5-10 seconds. The patient should feel the qi strongly go up the arm. Then remove the needle and have the patient mobilize the affected shoulder and evaluate therapeutic success. There can be substantial improvement.
Treatment III: Tuina and/or Needles
If the problem is directly at the shoulder joint, precisely at LI 15 (jianyu), two options are possible: tuina and needles. With the patient seated, vigorously rub LI 15 with a deep and rapid manipulation. The Chinese with whom I have studied tuina in Beijing say to rub this point 200 times in this manner. My experience is that most American patients cannot tolerate such a strong sensation for that length of time. Looking at them, I monitor how the treatment is affecting them and rub with a deep, precise, vigorous motion as long as I can. This may be only 20 seconds. Again, this technique is extremely strong, but it works very fast and is unequivocally efficacious for this type of shoulder pain. It is similar to the auricular treatment in that massage is used. It is ideal for frozen shoulder.
You may choose to needle LI 15 also. The point can be needled perpendicularly into the joint, or obliquely down the arm. Choose the perpendicular insertion if it is a joint problem, or an oblique insertion if upper arm muscles are involved. Insert the needles 1.0-1.5 inches perpendicularly, or obliquely and subcutaneously down the arm to the same depth and disperse the point. Even though needling unilaterally, this is a powerful needle technique and has a strong bearing down sensation. I find that patients prefer the tuina over the needle technique for this differentiation of shoulder pain.
Treatment IV: Threading
Finally, another classical Chinese option is threading ST 38 (tiaokou) to BL 57 (chengshan). BL 57 has the property of relaxing the muscle channels, and ST 38, close to ST 37 (shangguqu), the inferior he-sea point of the large intestine, has an effect on the shoulder. In combination, they assist in the treatment of shoulder pain.
Puncture ST 38 obliquely as you thread toward BL 57. Using a 2-3 inch needle, unilaterally insert to a depth of 1.0-1.5 inches on the right leg, since stomach/large intestine energetics are more right-sided as the pulse system shows. Even though the depth of insertion is relatively deep, this should not be a painful insertion. Using an insertion tube, simply tap the needle into the epidermis and then slowly insert to achieve the through-and-through technique. When you are in, keep manipulating the needle with a combined lift-and-thrust and wide amplitude technique. At this point, because you are deeply embedded in the musculature, the manipulation of the needle will feel heavy and sticky. This will produce a strong sensation in the leg. Let the patient know this. Manipulate the needle for half a minute or so, then remove it and have the patient mobilize the shoulder. Often there is significant improvement. This technique can be used for arthritis of the shoulder as well as peripheral inflammation of the shoulder.
In conclusion, these are simple yet comprehensive treatment strategies the practitioner can select from that have known clinical efficacy in the treatment of shoulder pain. Only one needs to be used. They work, the treatment is fast, and the results are long-lasting for the patient. As always, they are a testimony to the interrelatedness of body systems and the sagacity of Chinese medicine.
Point Location Reminders
LI 15: Anteroinferior to the acromion, in the middle of the upper portion of the muscle deltoideus. When the arm is in full abduction, the point is in the anterior depression of the two depressions appearing at the anterior border of the acromioclavicular joint.
LU 7: Superior to the styloid process of the radius, 1.5 cun above the transverse crease of the wrist (in the depression on the styloid process of the radius).
ST 38: Eight cun below ST 35, two cun below ST 37, midway between ST 37 and ST 41.
BL 57: Directly below the belly of the muscle gastrocnemius, on the line connecting BL 40 and the tendocalcaneous, about eight cun below BL 40.
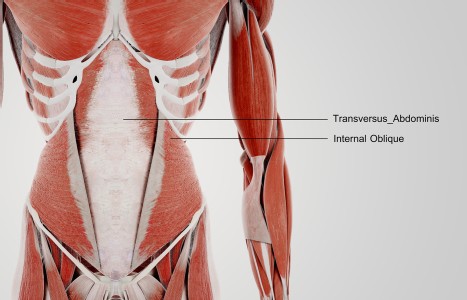
TrA-2, my primary needle location, I needle 95% of the time and I think it works the best. You’ll know you have the right point location when you discover the muscle twitching when applying electric stimulation.
Christopher Chapleau, DAc, LAc, Dipl. Ac., AIT, IMT, MSHP, CES, HMS
Microneedling has emerged as a widely embraced therapeutic modality for acupuncturists, offering diverse benefits ranging from addressing fine lines and wrinkles to treating conditions such as acne, acne scars, hair loss, melasma, and rosacea. This article focuses specifically on the application of microneedling as a therapy for acne and acne scars.
On Dec. 7, 2023, the World Health Organization (WHO) released its “Guideline for Non-Surgical Management of Chronic Primary Low Back Pain in Adults in Primary and Community Care Settings.”The purpose of the 244-page document is to “provide evidence-based recommendations on nonsurgical interventions for chronic primary LBP in adults” that will improve outcomes.