A Comprehensive Introduction to Abdominal Acupuncture
One morning in 1972, Dr. Zhi-yun Bo was treating a patient suffering from intense low back pain and sciatica that resisted improvement. A sudden inspiration reminded him that the Governing Vessel and the Conception Vessel are paired in a biao-li (Internal-External) relationship, and this moved him to try CV4 and 6. Within five minutes, the patient’s pain disappeared. Moreover, it never returned after only this one treatment. He repeated this point combination on several patients with similar conditions and was surprised to find the same results every time.
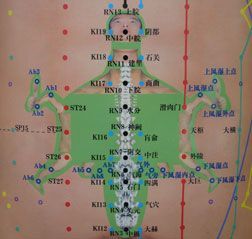
Thus, Dr. Bo began a 30-year exploration of the points of the abdomen that led to the discovery of what he believes is the Prenatal or Congenital Channel System that radiates from the umbilicus. He calls this system the Shen Que Channel System (SCS) because Shen Que (CV8) is the Chinese term for the umbilical acupoint. The SCS is the network of pathways that transports qi and blood from the mother to the fetus during gestation. Normal fetal development relies on the transportation and modulation of these essential substances from the mother before the fetus’ own zang fu organs produce them themselves. After birth, this system gradually integrates with the postnatal system whose qi and blood come from the zang fu organs generated from food essence. The SCS manifests as bands of points radiating from CV8. Because of its shape, it is likened to a tortoise and thus is called The Miraculous Tortoise.
Figure 1: Miraculous Tortoise: Shen Que Channel System (printed with permission from BMRIBA)
All parts of the body can be found in this system, and it is frequently used for musculoskeletal pain problems. An important characteristic of this system is that it is very close to the surface of the abdominal wall. Needles penetrating this system often lie on the surface of the abdomen with the tip just penetrating the skin. (The traditional 14 channel or postnatal system is slightly deeper in the adipose tissue.) Interestingly, the SCS possesses a strong capability to modulate the flow of qi and blood of the whole body and the effects of needling it are often instantaneous.
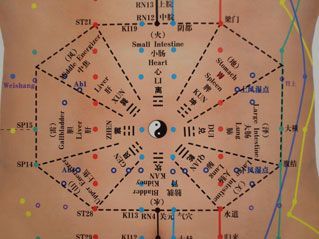
Dr. Bo also discovered that by needling deeper into the adipose and muscle layers of the abdomen, he was able to quickly harmonize the zang fu viscera. The layout of the organs matched that of the Post-Heaven Eight Trigrams (Ba Kuo) of the Book of Changes. The ancient diagram summarizes Dr. Bo’s clinical experience and establish a second system: The Zang Fu Organs System.
Figure 2: Ba Kuo Chart of Zang Fu Organs System
Because most of the organs or their biao-li pair resides in the abdomen, needling the zang fu can readily affect all the viscera. This is an advantage over using distal points on the extremities because it is not always easy for transmission of the stimulation from distal points to reach the organs, especially when there is a node-block higher up along the pathway that may require protracted periods of manipulation or additional needling in order to release the block.
At first glance, Bo’s Method of Abdominal Acupuncture (BMAA) might appear as just another microsystem. But “megasystem” might be the more appropriate description. It combines needling the prenatal channel system (Heaven level), the points of the postnatal system and extraordinary vessels on the belly (Humanity level), and the Zang Fu Organs System (Earth Level) establishing a multidimensional, comprehensive therapeutic system that harmonizes the viscera generating qi and blood, opens the regular 14 channels and Extraordinary Vessels, and pinpoints the anatomical locations of the problem to achieve an immediate, substantive and enduring healing effect. Furthermore, by using needles with gauges between 0.22 and 0.16, and with light manipulations and shallow insertion, it is virtually painless.
Dr. Bo integrated ideas from surgical procedures into his abdominal acupuncture system, manualized the application protocol in order to decrease learning time for students, improved efficacy and increased reproducibility in clinical trials. Some of attributes of his system include:
Standardization of point locations and locating methods: Points are located using a combination of anatomical landmarks and cun-ratios; they are measured by ruler and marked with a pen.
Manualized needle insertion/manipulation procedure: Practitioners stand on the right side of the patient and insert needles from top to bottom, deep to shallow, inside to outside. Likewise, needle length and gauge are standardized based upon patient size and weight, deficiency or excess condition, and type of disease.
Standardized point formulas: There are more than 20 pattern-based, disease-focused, standardized point formulas for the most common diseases seen in acupuncture clinics.
Integration of Western diagnostics: The physical exam is used for musculoskeletal problems and stroke recovery; biomedicine tests are consulted for internal medicine conditions; and when appropriate, objective testing is used to assess clinical efficacy. In this way, Western techniques and technology are integrated into BMAA’s diagnostic model.
The creation of standardized point formulas is based upon their effectiveness in more than 30 years of clinical experience. These formulas are supplemented with additional points to individualize them for specific patients and can be combined for more complex cases. For example, in cervical spondylosis with nerve-root compression presenting with pain in the neck and shoulders, and numbness in the hands, CV12 and 4 are used to generate qi and blood from the spleen and kidney (govern muscles and bones). K17 and 18 bilaterally are used to relax the muscles of neck and free the nerve roots. ST24 bilaterally is used to guide qi and blood into the upper extremities (yang ming: copious qi and blood). The Superior Wind-Rheum point (Ab1) and Superior-Lateral Wind-Rheum point (Ab2) are used on the affected side to pinpoint numbness affecting the hand(s) while dispelling wind and dampness from the channels. Depending on the location of nerve compression, the location of K18 can be adjusted or additional points like Superior-CV10 can be used.
Current Usage and Status in China
In 1991, BMAA won an acupuncture and tui na techniques competition organized by the Shanxi Regional Ministry of Health. Dr. Bo formally introduced his system to the public in 1992. In 2007, it was recognized as a professional subcommittee under the China Acupuncture and Moxabustion Association.1 Indications include: orthopedic problems, respiratory infections, coronary artery disease, hypertension, digestive problems, neurological conditions, gynecological problems, and difficult-to-treat diseases like Parkinson’s, insomnia, depression, diabetes mellitus, eye diseases, obesity, deafness and tinnitus.2
In Beijing, many acupuncture doctors and professors use BMAA. Dr. Bo’s apprentices run several stroke recovery centers using this therapy as the primary treatment. Dr. Bo successfully treated Guangdong First Provincial Hospital of Traditional Chinese Medicine staff members who suffered from necrosis of the trochanter (a side effect from steroid treatment for SARS infections). BMAA is now the principle treatment method used in the hospital, and the department heads of cardiology, gynecology, emergency medicine, acupuncture, orthopedics and the traditional medicine center are all his apprentices.
Current Research
According to a systematic review using a Chinese academic search engine, Wang et al. found that from 1999-2007, 214 articles have been published on BMAA in China, including 96 clinical trials, of which 62 used comparative treatment for control groups.3-4 Of the 74 musculoskeletal diseases studied, 30 were for cervical spondylosis with nerve-root compression. Of those, 22 used comparative treatment control groups. Efficacy was more than 90 percent. Among the 22 studies, a multi-site study was conducted in 2005 at three hospitals, in which 300 subjects were randomized into BMAA and traction therapy treatment groups. Traction therapy was found to “improve local blood circulation and relieve symptoms but lacked stable, long-term, curative effects which lead to frequent relapses,” while the cure rate with BMAA reached 91.5 percent (complete remission within 10 treatments and no return for three months) and an efficacy rate of 98 percent.5
Student Training
The BMAA training program is carried out over a three year period.
First year (five-day course): Learning and practicing point location on the Miraculous Tortoise; training in the needle insertion protocol; use of the BMAA formulas for musculoskeletal pain problems.
Second year (four-day course): Refining point location and needle insertion protocol skills; deepening understanding of location depths; discussion of SCS theory in depth; advanced topics in first-year diseases; introduction of internal-medicine diseases, cerebral vascular disease and stroke recovery.
Third year (two-day course; one-month apprenticeship training): Review and deepening of theory and diseases of second-year; apprenticeship training for pattern differentiation mastery and technique refinement.6
In Dr. Bo’s lineage, the arrival of qi is felt by the practitioner, not necessarily the patient. It requires a sensitivity to needle sensation that must be cultivated with a mentor. As Prof. Bo’s apprentices establish teaching and research centers outside of China, more courses will become available.
References
First BMAA Academic Symposium at the First Guangdong Provincial Hospital of TCM. Guangzhou, China; March 2007.
Ryan P. Integration of modern and traditional teaching methodologies in abdominal acupuncture training. Conference Proceedings of the First Academic Symposium on Abdominal Acupuncture, Guangzhou 2007:205.
Mast cell activation syndrome (MCAS) affects more than 15% of the U.S. population but evades most practitioners’ radar. Just five years ago, it wasn’t even on my radar, despite already having 20 years of experience as a clinician at that time. The more I dug (similar to leaky gut and post-COVID syndrome), the more I found my patients were suffering from this disorder.
Research supports the effectiveness of selecting the distal acupuncture points for the treatment of microtrauma and for relieving pain, particularly in cases of chronic shoulder pain. But to make the treatment results long-lasting, clinical experience and research suggest that instead of treating the most painful structure first, we identify the inhibited driver, restore reliable recruitment, confirm it with immediate re-testing, and only then address the painful area as a branch of a deeper pattern.
The motivation behind our practice of medicine is important, impacting not just our experience but also the experiences of those we treat. It is perhaps for this reason that the aspiration to help not just some, but all beings heal, has historically been an important part of the medical tradition. To explain this, we need to consider how medicine is interwoven with other social domains.