Douglas R. Briggs, DC, Dipl. Ac. (IAMA), DAAPM, EMT
The patient came into my office with the classic antalgic stoop. She was bent over almost to ninety degrees, leaning on her husband for support and staggering to walk. She had been under supportive care for a long time, but this new pain scared her. She had called her family doctor and been told it was sciatica and she already had a referral to a back surgeon – after all, a previous MRI had shown disc bulges. Even though we had been able to maintain her back for a long time, she was sure she would need surgery just because of the intense pain. The reason she came to me was to help with the pain, as she could not get in with the surgeon for another week. We helped her back to the treatment room and onto the table.
As I ran through the consult, she localized the pain to her right middle buttock – but the pain spread out across the lower back and down the leg. Pretty much all of the orthopedic tests I tried were positive immediately, and soft tissue palpation was highly sensitive across the region. The big telling sign was the position of her leg – not only was her right leg pulling up shorter, but her foot was rotated almost totally to the side. We were dealing with a piriformis spasm.
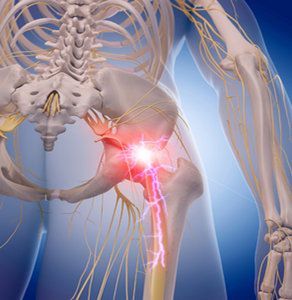
The piriformis muscle typically attaches medially to the anterior of the sacrum, and laterally to the greater trochanter. In most people, it is a thick and bulky muscle and the sciatic nerve runs either over, under, or through the muscle. When in spasm, the trigger point is usually at either the sacral attachment or in the belly of the muscle. Pain pattern is typically across the buttock and down the back of the thigh – spreading out with increased spasm in the muscle. This spasm will often contribute to the finding of a functional short leg.
A muscle spasm can mimic any number of other conditions, including disc rupture and nerve root injury. From a pain management perspective, it is often the absence of significant bony, disc, and nerve pathology that helps direct the clinician toward a diagnosis of myofascial pain. As chiropractors, we pay more attention to the musculoskeletal arrangement and are more likely to pick up on a muscle spasm than a family doctor who notes a history of a disc bulge. But even with positive diagnostic studies, you cannot rule out a diagnosis of myofascial spasm - in fact, myofascial spasm is a frequent basis of acute and chronic pain in any muscle location of the body. All of the classic "tender points" of fibromyalgia can be attributed to muscle spasm, as a quick look at any trigger point chart will confirm.
Piriformis syndrome is a specific named syndrome for the pain caused by spasm in the piriformis muscle – it can produce symptoms as common as pain in the lower back, groin, perineum, buttock, hip, posterior thigh, leg and foot, and also increased pain in the back and rectum with bearing down. In severe cases, the patient may also have swelling in the painful limb and even sexual dysfunction.
After the classical pain pattern, the position of the leg is the most common indicator of piriformis syndrome. It is a simple check for outward rotation of the foot on the involved side. In my experience, this may be observed in either the prone or supine position, but most often prone as patients are more comfortable face down. Palpation over the belly of the piriformis (near GB30) is often acutely tender and will produce a "jump sign" when goaded. The combination of pain in the sciatic distribution and hip rotation discussed above is referred to as Bonnet's sign. The sacrum may be rotated forward on the side of spasm - giving a positive Webster's sign and restriction the normal fluid motion of the SI joint.
There are several considerations when treating a piriformis syndrome. Although some form of therapy is necessary, in many cases the patient will not tolerate aggressive trigger point work on the muscle right away. Acupuncture is a great way to release the spasm and alleviate the pain. Of course, if you are dealing with a muscle problem, then a joint dysfunction is most likely implicated – I will certainly recommend a referral to a chiropractor to evaluate for and correct any subluxations in the pelvis – this will only enhance the benefit of your care and help the patient.
When a patient presents with any category of lower back or pelvic pain, I always check the piriformis. It's too easy to take a quick look at the relative position of the feet to not include it in my overall assessment. If there is a piriformis spasm, I use the standard Nimmo protocol with great results. As for my patient who came in with back pain – we were able to get her pain down by 50% just doing needles over the ashi points with EMS and some light myofascial work that first day. She rested at home with ice that evening and we were able to get very good motion into the sacroiliac joint the next day. She did follow up with the surgeon, who opted to cancel the surgery as her problems had resolved – even with a history of a disc bulge, she had no pain or positive neurological findings.
As always, remember to document your findings, treatment, and the patients' response to care – as this only serves to bolster your professional credibility and your reputation as a physician and a healer.
Mast cell activation syndrome (MCAS) affects more than 15% of the U.S. population but evades most practitioners’ radar. Just five years ago, it wasn’t even on my radar, despite already having 20 years of experience as a clinician at that time. The more I dug (similar to leaky gut and post-COVID syndrome), the more I found my patients were suffering from this disorder.
Research supports the effectiveness of selecting the distal acupuncture points for the treatment of microtrauma and for relieving pain, particularly in cases of chronic shoulder pain. But to make the treatment results long-lasting, clinical experience and research suggest that instead of treating the most painful structure first, we identify the inhibited driver, restore reliable recruitment, confirm it with immediate re-testing, and only then address the painful area as a branch of a deeper pattern.
The motivation behind our practice of medicine is important, impacting not just our experience but also the experiences of those we treat. It is perhaps for this reason that the aspiration to help not just some, but all beings heal, has historically been an important part of the medical tradition. To explain this, we need to consider how medicine is interwoven with other social domains.