Tight Hip Flexors and Painful Arthritis: The Surprising Connection
Thomas Michaud, DC
| DIGITAL EXCLUSIVE
You would think the connection between hip arthritis and pain would be pretty straightforward: People with the greatest degree of arthritis as measured on X-rays should have the greatest amount of pain. Surprisingly, this is not always the case, as many people with severe arthritis are relatively asymptomatic, while people with slight arthritis present with disabling pain.
In an attempt to understand exactly why an arthritic hip hurts, researchers from London implanted special pressure sensors inside the hips of 50 individuals as they were undergoing hip replacement surgery.1 Prior to surgery, each patient filled out a detailed questionnaire to precisely quantify the severity of their pain, with zero representing no pain and 10 signifying "the worst imaginable pain."
During the surgery, surgeons moved their patients' hips through full ranges of motion in all directions while measuring pressure changes within the hip joint. After completing their evaluation, they noted a significant linear correlation between elevated intra-articular pressure and pain: People with the highest pressures had the greatest amount of pain.
The researchers also noted that hip extension and internal rotation nearly doubled the resting pressure within the hip joint and was strongly correlated with the presence of preoperative pain.
A Problem of Pressure and Tension
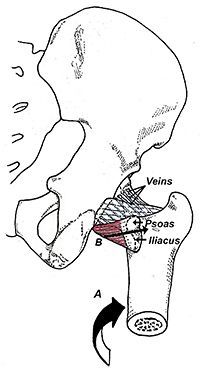
FIG 1 Venous drainage of the hip. Extension and internal rotation of the femur (A) increases tensile strain in the iliopsoas muscle (B), causing its tendon to compress the long, narrow veins traversing the femoral neck. Compressing these veins impairs venous drainage, resulting in increased intra-articular hip pressure.
The reason hip extension and internal rotation markedly elevate hip pressures is because the iliopsoas tendon sits directly on top of a series of small veins that traverse the femoral neck. When the hip is extended and/or internally rotated, the iliopsoas tendon compresses these veins and the impaired venous drainage results in increased intra-articular hip pressure (Fig. 1).
Interestingly, the study authors emphasize that the first movements lost with hip arthritis are extension and internal rotation, and that these motions are restored after the induction of anesthesia – confirming that it is not the joint capsule or arthritis that is limiting these motions, but tension in the hip flexors.
The authors also state that the connection between iliopsoas tension and hip pain is supported by the observation that surgically lengthening the iliopsoas tendon produces dramatic reductions in hip pain.
In addition to producing pain before hip replacement, tension in the hip flexors is also a common cause of pain following hip replacement, but for a different reason. Following hip replacement, when the hip flexors are tight, the iliopsoas tendon compresses directly against the new prosthetic cup, often fraying the undersurface of the tendon. This would not happen if the hip flexors were loose.
This is especially problematic in small individuals, as surgeons typically use the largest acetabular cup possible to prevent the risk of hip dislocation following surgery.
Fraying of the iliopsoas tendon against the acetabular cup is often difficult to diagnose, since MRI imaging is not possible, as the metal femoral head and neck prevent adequate imaging; diagnosis is usually confirmed with expensive diagnostic pain blocks.
An Exercise / Stretching Protocol
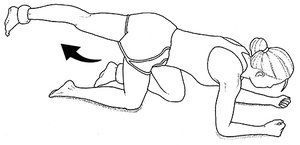
FIG 2 Gluteus maximus kickbacks.
Rather than sending out for testing, I personally just assume that pain near the anterior aspect of the acetabular cup following total hip replacement is due to tension in the iliopsoas, and I prescribe specific exercises and stretches to address the problem.
In my experience, the most effective ways to lengthen iliopsoas is to produce reciprocal inhibition of the hip flexors by fatiguing the hip extensors prior to stretching the iliopsoas. To do this, have the patient get on all fours and do kickbacks to fatigue (Fig. 2). If the patient can do more than 30 of these without tiring, place an ankle weight on so that fatigue occurs with fewer than 30 repetitions.
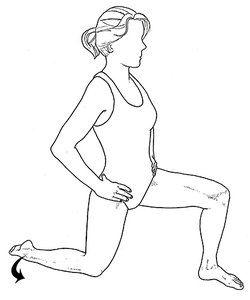
FIG 3 Hip flexor stretch. The degree of stretch placed on the iliopsoas muscle can be increased by kicking the involved ankle outwardly (arrow), thereby internally rotating the hip.
After the gluteus maximus is exhausted, immediately stretch the hip flexors with the standard hip flexor illustrated in Figure 3.
To really target the iliopsoas, internally rotate the extended femur by moving the foot laterally. Moving the foot laterally increases strain on the iliopsoas, allowing for a more effective stretch. I have the patient repeat the stretch 10 times daily, holding each stretch for 60-90 seconds.
Interesting new research shows that it is possible to physically lengthen a muscle by holding static stretches for prolonged periods of time.2 The same prolonged static stretches have also been shown to improve tendon resiliency, which may reduce tension in the iliopsoas tendon as it passes over the iliopectineal eminence and femoral neck.
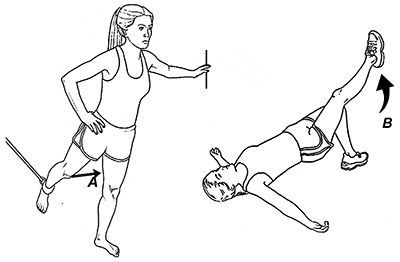
FIG 4 Hip flexor home exercises. With resistance provided by an anchored band, the hip flexors are exercised by driving the knee up and forward (A). An alternate method to strengthen the hip flexors is to raise and lower the straight lower extremity while performing a supine bridge (B). It is important to maintain the pelvis in a fixed position while performing this exercise.
In many situations, a chronically tight iliopsoas needs to be strengthened as well as stretched, as a weak muscle stiffens in response to being overloaded. The easiest way to strengthen the iliopsoas is with the exercises illustrated in Figure 4. Three sets of 15 repetitions performed three times a week are usually more than enough to strengthen the iliopsoas.
Of course, to prevent the hip flexors from shortening throughout the day, make sure the patient avoids prolonged sitting, and recommend switching to a standing desk if possible. Also make sure the patient is not sleeping in a fetal position, which places the iliopsoas in a shortened position, making it difficult to lengthen with even the most aggressive stretching protocols.
References
Goodard N, Gosling P. Intraarticular fluid pressure and pain in osteoarthritis of the hip. J Bone Joint Surg (Br), 1988;70-B:52-55.
Panid L, Bogdanis G, Terziz G, et al. Muscle architectural and functional adaptations following 12-weeks of stretching in adolescent female athletes. Front Physiol, July 2021;12:701338.
Mast cell activation syndrome (MCAS) affects more than 15% of the U.S. population but evades most practitioners’ radar. Just five years ago, it wasn’t even on my radar, despite already having 20 years of experience as a clinician at that time. The more I dug (similar to leaky gut and post-COVID syndrome), the more I found my patients were suffering from this disorder.
Research supports the effectiveness of selecting the distal acupuncture points for the treatment of microtrauma and for relieving pain, particularly in cases of chronic shoulder pain. But to make the treatment results long-lasting, clinical experience and research suggest that instead of treating the most painful structure first, we identify the inhibited driver, restore reliable recruitment, confirm it with immediate re-testing, and only then address the painful area as a branch of a deeper pattern.
The motivation behind our practice of medicine is important, impacting not just our experience but also the experiences of those we treat. It is perhaps for this reason that the aspiration to help not just some, but all beings heal, has historically been an important part of the medical tradition. To explain this, we need to consider how medicine is interwoven with other social domains.