Exercising the Multifidi: Why Isometric Contractions Are Essential
And a great exercise protocol to help your patients.
Thomas Michaud, DC
| DIGITAL EXCLUSIVE
WHAT YOU NEED TO KNOW
From the Latin term for "many," the multifidi muscles have more than twice the cross-sectional area of the surface erector spinae, which allows them to generate a powerful stabilizing force in the lumbar spine.
Research shows that exercises incorporating the isometric contractions produced hypertrophy of the multifidi. Conventional exercises produced no change in multifidus volume.
It makes sense that patient outcomes would improve when the prescribed exercises accurately target the specific muscles proven to correlate with chronic low back pain.
In any given year, nearly 40 percent of the U.S. population will develop a low back injury severe enough to limit activity.1 Once injured, there is a 22 percent chance of reinjury within three months and a nearly 80 percent chance of reinjury within the next three years.2
The cost of treating these injuries is astronomical: In 2013, $87.6 billion was spent on the management of low back pain, making it the third most expensive health care condition behind diabetes and ischemic heart disease.3
Over the past 40 years, traditional diagnostic approaches have focused on using high-tech imaging to identify specific pain source generators; e.g., herniated discs, sacroiliac abnormalities and/or osteoarthritis of the lumbar spine. Unfortunately, this approach has failed to establish a consistent relationship between specific anatomical variants and pain, since asymptomatic people often present with disc herniations,4 and spinal osteoarthritis has little correlation with pain.5
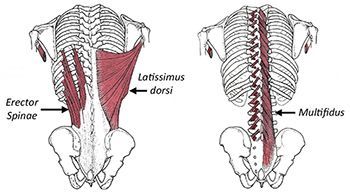
FIG 1 Superficial and deep muscles of the lumbar spine. The deep fibers of the multifidi span two vertebral segments, while the superficial fibers of the multifidi traverse 2-5 levels before reattaching. Because they span such short distances, the multifidi essentially behave as variable length ligaments and play an important role in fine-tuning subtle perturbations in joint motion.
While imaging studies have been proven to be poor predictors of back pain, research dating back to the mid-1970s shows that compared to similarly aged controls, patients with low back pain present with atrophy and increased fatty infiltration of the multifidi muscles.6 From the Latin term for "many," these interesting muscles have more than twice the cross-sectional area of the surface erector spinae, which allows the multifidi to generate a powerful stabilizing force in the lumbar spine. (Fig. 1)
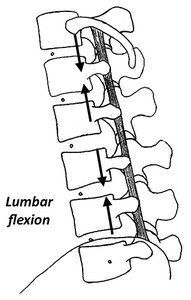
Significantly, the multifidi generate peak force output when the spine is fully flexed,7 which is extremely important for maintaining spinal stability, as low back injuries are more likely to occur when the spine is flexed. The multifidi are capable of creating this force because their deep fibers lie close to the spine's axis of motion, which allows them to compress the spine, rather than extend it. (Fig. 2)
FIG 2 Because of their anterior location, the deep fibers of the multifidi create a compressive force when the lumbar spine is flexed (arrows).
In addition to their reduced volume, the multifidi muscles in low back pain patients even fire differently. EMG studies by MacDonald, et al.,8 show the multifidi in people with low back pain have significant delays in activation when the spine is loaded, and the deep fibers have a diminished response to protecting against anticipated movements. Without the multifidi creating a protective compressive force, the lumbar spine could be injured with even subtle spinal movements.
All these reasons explain why Ward, et al.,9 claim that the multifidi are key stabilizers of the lumbar spine, and that atrophy and/or impaired function of these muscles will have a profound effect on spinal degeneration.
It is possible to evaluate the ability of the multifidi to create a compressive force in the lumbar spine by using the prone hip extension / knee flexion test.10 To perform this test, position the patient prone on an examining table and say: "Tense both buttock muscles and maintain this contraction for the duration of the test. Now bend one knee to 90° and lift that knee off the table."
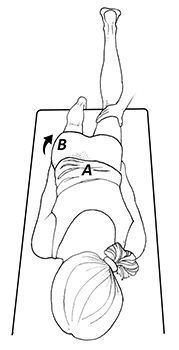
FIG 3 Prone hip extension / knee flexion test. I've modified the original test used by Hughes, et al.,9 in that I push down with light pressure on the back of the involved knee. I find the added pressure helps identify even slight weakness of the multifidi.
Ideally, when the deep multifidi are creating a stabilizing compressive force in the lumbar spine, the pelvis remains still and the lumbar spine keeps its neutral alignment. In contrast, when the multifidi are weak, the deep fibers fail to lock the lumbar vertebrae and the entire lumbar spine arches as the surface erector spinae muscles extend the low back (Fig. 3A). In cases of extreme multifidi weakness, the opposite pelvis often lifts off the table (Fig. 3B).
In a recent study of 50 elite-level rugby players evaluated with the prone hip extension / knee flexion test, Hughes, et al.,10 demonstrate that excessive arching of the lumbar spine while performing this test markedly increases the risk of not just low back injury, but also injury to the hip, pelvis, hamstrings, and/or calves.
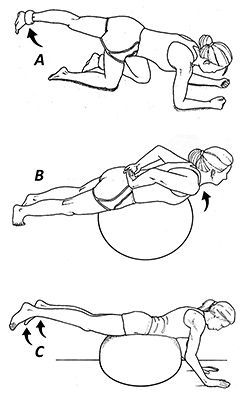
Although there are many exercises that theoretically target the multifidi, my favorite way to increase multifidus volume and improve function is with the exercises illustrated in Fig. 4. When performing these exercises, it is essential to perform a five-second isometric contraction at the end of each repetition.
FIG 4 Common multifidus exercises. A) Leg extension in four-point kneeling. B) Prone trunk extension. C) Bilateral prone leg lifts. Note that only exercises incorporating isometric contractions produce hypertrophy of the multifidi (see text).
In an important study from Belgium,11 researchers used CT scans to measure volume of the multifidi before and after a 10-week exercise program. Three different exercise routines were evaluated: progressive stabilization exercises; three sets of 15 reps of the exercises illustrated in figure 4 performed without isometric contractions; and the same exercises performed with five-second isometric contractions at the end of each repetition.
At the end of the study, the authors demonstrated that only the exercises incorporating the isometric contractions produced hypertrophy of the multifidi. Conventional exercises produced no change in multifidus volume.
Recent research shows that isometric contractions work in a manner similar to blood flow restriction training in that the increased intramuscular pressure associated with isometric contractions impairs intramuscular blood flow, which in turn increases recruitment of fast-twitch muscle fibers, increases the production of growth hormone, and even promotes the formation of vascular endothelial growth factor.12
The latter is important as a recent histological study confirmed that people with low back pain have reduced vascularity in their multifidi,13 and vascular endothelial growth factor would help promote the formation of new blood vessels.
While performing these exercises, it is important to use verbal and physical cueing of the multifidi to enhance recruitment. Beneck, et al.,14 demonstrated that simply saying, "Push your tailbone backward to tighten your low back muscles" as participants performed conventional low back exercises, markedly increased EMG activity in the multifidi.
In addition to verbal cues, I always incorporate a physical cue in which I place my thumbs on the paraspinals over the sacrum, and my index and middle finger over the paraspinals adjacent to L3. As I give the verbal cue to tighten the low back muscles, I squeeze my thumbs and index fingers together, instructing the patient to focus on tightening the back muscles between my fingers. The physical cue is especially effective with asymmetric atrophy of the multifidi.
I've been using both verbal and physical cues for the past two years and have been surprised by how effective this approach is, even with the most recalcitrant low back pain patients. It makes sense that patient outcomes would improve when the prescribed exercises accurately target the specific muscles proven to correlate with chronic low back pain.
References
Hoy D, Bain C, Williams G, et al. A systematic review of the global prevalence of low back pain. Arthritis Rheum, 2012;64:2028-2037.
da Silva T, Mills K, Brown BT, et al. Risk of recurrence of low back pain: a systematic review. J Orthop Sports Phys Ther, 2017;47:305-313.
Dieleman JL, Baral R, Birger M, et al. US spending on personal health care and public health, 1996-2013. JAMA, 2016;316:2627-2646.
Nakashima H, Yukawa Y, Suda K, et al. Abnormal findings on magnetic resonance images of the cervical spines in 1211 asymptomatic subjects. Spine, 2015;40:392-398.
Brinjikji W, Luetmer P, Comstock B, et al. Systematic literature review of imaging features of spinal degeneration in asymptomatic populations. Am J Neuroradiol, April 2015, 36 (4) 811-816.
Shahidi B, Parra CL, Berry DB, et al. Contribution of lumbar spine pathology and age to paraspinal muscle size and fatty infiltration. Spine, 2017;42:616-23.
Ward SR, Kim CW, Eng CM, et al. Architectural analysis and intraoperative measurements demonstrate the unique design of the multifidus muscle for lumbar spine stability. J Bone Joint Surg Am, 2009;91:176-185.
MacDonald D, Moseley GL, Hodges PW. People with recurrent low back pain respond differently to trunk loading despite remission from symptoms. Spine, 2010;35:818-824.
Ward S, Kim C, Eng C, et al. Architectural analysis and intraoperative measurements demonstrate the unique design of the multifidus muscle for lumbar spine stability. J Bone J Surg Ser A, 2009;91:176-85.
Hughes R, Cross M, Stokes K, et al. Novel biomechanical injury risk score demonstrates correlation with lower limb posterior chain injury in 50 elite- level rugby union athletes. BMJ Open Sport & Exer Med, 2021;7:e001062.
Daneels L, Vanderstraten G, Cambier D, et al. Effects of 3 different training modalities on the cross-sectional area of the lumbar multifidus muscles in patients with chronic low back pain. Br J Sports Med, 2001;35:186-191.
Conceicao M, Junior E, Telles G, et al. Augmented anabolic responses after 8-week cycling with blood flow restriction. Med Sci Sports Exerc, 2019;51:84-93.
Padwal J, Berry D, Hubbard J, et al. Regional differences between superficial and deep lumbar multifidus in patients with chronic lumbar spine pathology. BMC Musculoskel Disor, 2020;21:764.
Beneck G, Story J, Donald S. Postural cueing to increase lumbar lordosis increases lumbar multifidus activation drink trunk stabilization exercises: electromyogram fig assessment using intramuscular electrodes. J Orthop Sports Phys Ther, 2016;46:293-299.
Chronic pain afflicts over 20% of the adult population. Sadly, most MDs have essentially no education in treating pain, beyond offering a few toxic medications. Then they tend to steer people with pain away from those health practitioners who are trained. This puts the acupuncture community on the front lines for addressing this epidemic.
When the body is going through a stressful event, the sympathetic system is activated. This activation will help the body with a life-threatening situation. If this state is activated for prolonged periods of time, it starts to consume energy. These traumatic events that generate stressors in the autonomic nervous system (ANS) will eventually become internalized.
One of the things that makes acupuncture so difficult to measure is that the medicine actually does contain some esoteric aspects. There have been numerous studies that demonstrate the neurochemical reasoning behind why acupuncture points stimulate the autonomic nervous system to enact change However, not all the benefits of TCM can easily be measured by randomized, controlled trials. But does that make them fundamentally and definitively untrue?