The Five-Element Course of Symptom Transmission (CST)
Eric M. Hao, MSAOM, LAc
The CST is an overlooked and rarely discussed TCM subject. The Five-Element sequence discloses information for the diagnosis and prediction of symptom transmission of neck injuries when examined using an anatomical and meridian map of the neck area.
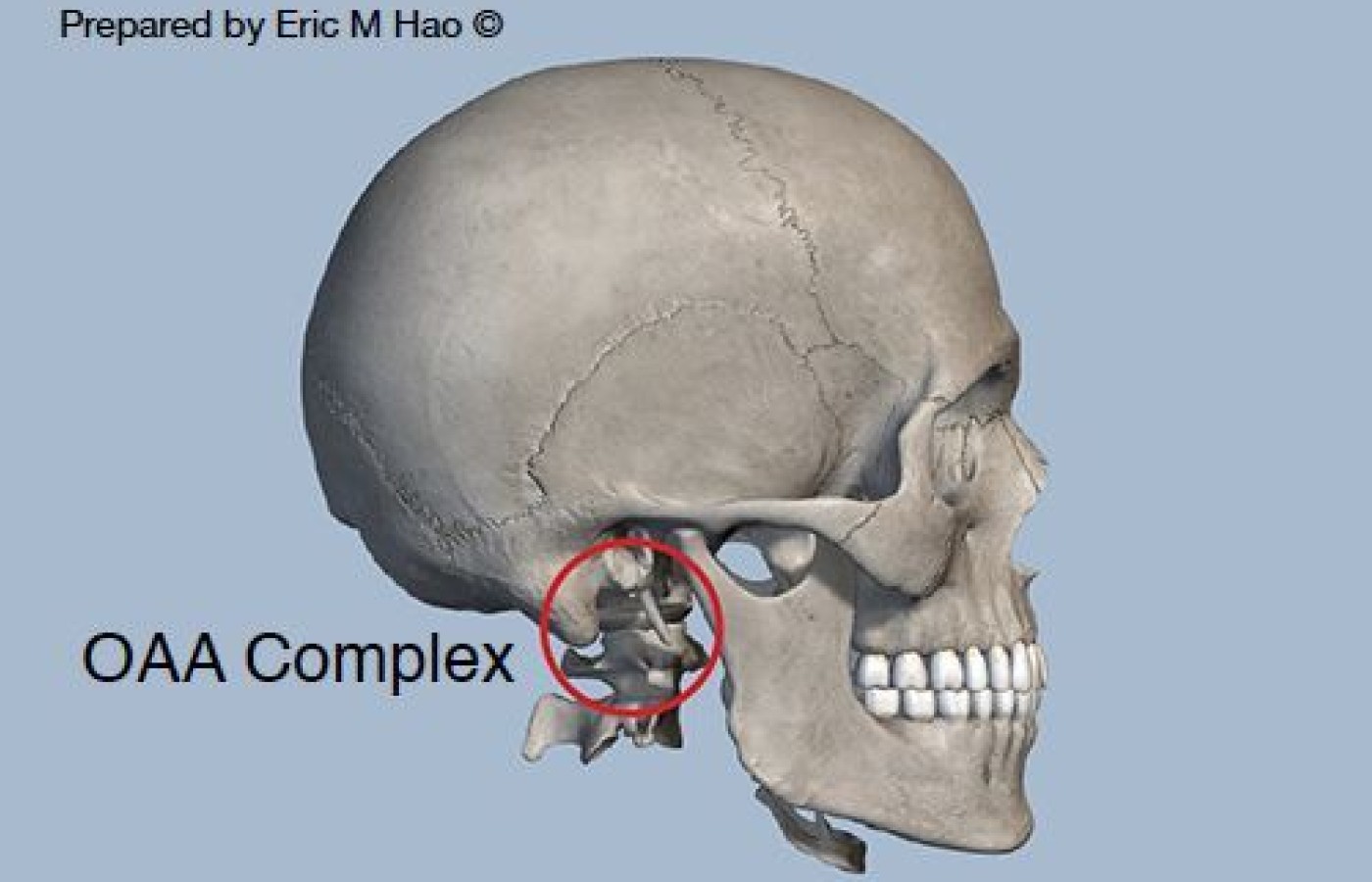
In Figure 2, the Occipital bone, Atlas, and Axis (OAA) complex is responsible for the range of motion of the head and functions as the weight-bearing structure of the cranium.33 It supports the globe of the head and serves as a hinge on which all of the vital tissues (e.g., spinal cord and blood vessels) can retain the physiological curvatures within a normal range when entering the skull.
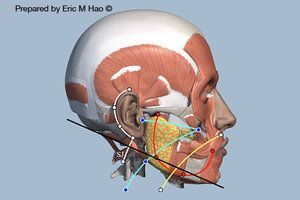
Fig. 3. The meridian map and CST in the neck. The bony level of the OAA complex is mapped onto the soft tissue by a line that connects the cranial base and the lowest point of the chin to delineate the head and neck. A new CST was discovered by matching this line with the meridian courses in the neck area showing that SanJiao (SJ, white) comes before Small Intestine (SI, blue).
The OAA complex is susceptible to incorrect alignment with the head and can cause neuromuscular and sensorimotor symptoms34 or, in Chinese medicine, block the free flow of Qi, blood, and meridians, resulting in symptoms in the neck, shoulders, and arms. Due to its anatomical significance, the level of the OAA complex plays a vital role in the CST among the meridians in Chinese medicine when examining the five-element sequence from an anatomical perspective.
The skull consists of the cranial and facial bones. Since the level of the OAA complex is not visible in the soft tissue, a reference line serves as the bony level of the complex to be mapped onto the soft tissue in the neck area is required to reveal the actual CST among the meridians (Figure 3).
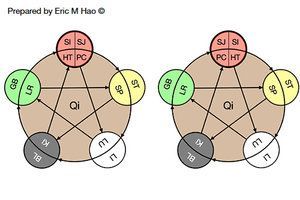
Fig. 4. The traditional (left) vs the modified (right) five-element model. The key difference between the two is in the sequence of SanJiao/Pericardium (SJ/PC), which comes before the Small Intestine/Heart (SI/HT) in the modified model (bolded black circles). It was discovered by incorporating a "meridian map" in the neck area at the level of the bony OAA complex to verify the CST of neck disorders.
A line that connects the cranial base (the lowest point of the cranial bones) and the lowest point of the chin (the lowest point of the facial bones) form the inferior border of the skull and demarcate the head and neck on the bony structures. When mapping the line onto the soft tissue, it intersects with the "meridian map" in the neck area.
The mapping shows the anteroposterior relationship among the meridians in a specific order starting from the BL (Bladder), GB (Gallbladder), SJ (SanJiao/Triple Heater), SI (Small Intestine), ST (Stomach), to the LI (Large Intestine). The new sequence differs from the traditional Five-Element model in that the SJ/PC meridians come before the SI/HT meridians (Figure 4).
The sequence revealed by using the bony and soft tissue anatomy is compatible with clinical manifestations of WAD and neck injury patients. As pointed out previously, the corrected Five-Element model provides the information of diagnosis, prediction of the symptom transmission, and the accurate treatment sequences.
Merging the New Theory with Western Medicine
Science is the core value of Western medicine and is the basis for advancements in medical technology. It guides clinical practice and is the main reason why Western medicine dominated the field and overcame TCM despite the latter's longevity.
The human body is a compact version of nature and continually adapting to changes. Over the long term, nature has more profound impacts on human lives than science. It is equally important not to overlook the body's natural healing ability while searching for scientific answers regarding the complexity of human structure.
In the revised TCM theory, the prime concern is not "nature vs. science" or "Chinese vs. Western medicine." It is about finding a way to best use the power of nature, connect it to science, and "blend" them harmoniously. In other words, the purpose is enhancing the quality of theories and integrating techniques with Western medicine to achieve goals that have not yet been accomplished.
Discussion
If the inadequate foundations of TCM theory are perceptible by applying natural phenomena and medical knowledge and yet its purveyors choose to neglect the facts, this will prevent Chinese medicine and acupuncture from further improvement.
One opinion asserts that traditional Chinese medicine is no longer traditional once its foundations and theories are modified. This disputable viewpoint is not sustained when tracing China's medicinal records. The properties of several Chinese herbs, including Ginseng, have changed many times according to findings from continuous clinical practice.35 If Materia Medica, considered the bible of Chinese herbology, is revisable when errors occur, the same should apply to TCM foundations and theories.
Some have questioned the bases for the modified acupuncture system to claim better effectiveness than traditional acupuncture for the management of intractable pain and numbness. The answers lie in the modified theory that aligns with nature and the evidence-based clinical results of more than 25,000 cases worldwide. The ancient Chinese implemented their observations and experiences from the oldest form and the largest scale of human subject research as the foundation of TCM. Thus, TCM and acupuncture practitioners' have a duty to fortify the integrity and wholeness of the theoretical frame-works when new findings are discovered and verified in practice.
Eastern and Western medicine view and approach the human body differently to understand disease prevention and treatment. Both have pros and cons. In my opinion correcting errors and preventing mistakes are two essential criteria that are more important than innovation in medical practice.
References
33. Swartz EE, et al. Cervical spine functional anatomy and the biomechanics of injury due to compressive loading. Journal of Athletic Training, 2005; 40, 155–161.
34. Sterling M. Whiplash-associated disorder: musculoskeletal pain and related clinical findings. The Journal of Manual & Manipulative Therapy, 2013; 19, 194-200.
35. Chang TM. (1997). Chinese herbology, lecture 8. The properties of herbs (Chinese). The Qi, 1997.
Editor's Note: The previous article in this series appeared in the August issue.
Mast cell activation syndrome (MCAS) affects more than 15% of the U.S. population but evades most practitioners’ radar. Just five years ago, it wasn’t even on my radar, despite already having 20 years of experience as a clinician at that time. The more I dug (similar to leaky gut and post-COVID syndrome), the more I found my patients were suffering from this disorder.
Research supports the effectiveness of selecting the distal acupuncture points for the treatment of microtrauma and for relieving pain, particularly in cases of chronic shoulder pain. But to make the treatment results long-lasting, clinical experience and research suggest that instead of treating the most painful structure first, we identify the inhibited driver, restore reliable recruitment, confirm it with immediate re-testing, and only then address the painful area as a branch of a deeper pattern.
The motivation behind our practice of medicine is important, impacting not just our experience but also the experiences of those we treat. It is perhaps for this reason that the aspiration to help not just some, but all beings heal, has historically been an important part of the medical tradition. To explain this, we need to consider how medicine is interwoven with other social domains.