We Need a Better Way to Conceptualize Viral Infections (Pt. 2)
Immune Profiles, Supplementation and the Acupuncturist's Opportunity
David Seaman, DC, MS, DABCN
| DIGITAL EXCLUSIVE
WHAT YOU NEED TO KNOW
The immune profiles of obese individuals are reflective of that of a viral infection state, as if the immune system is primed and ready to act.
So, it is not surprising why obese people suffer more from acute respiratory infections than non-obese people.
I am not disputing that we can transmit infectious diseases; however, it does seem that most of our typical “infectious events” are disruptions in an individual’s personal homeostatic relationship with the 3 quadrillion viruses in their body.
Editor’s Note: Pt. 1 of this article ran in the September issue (digital exclusive).
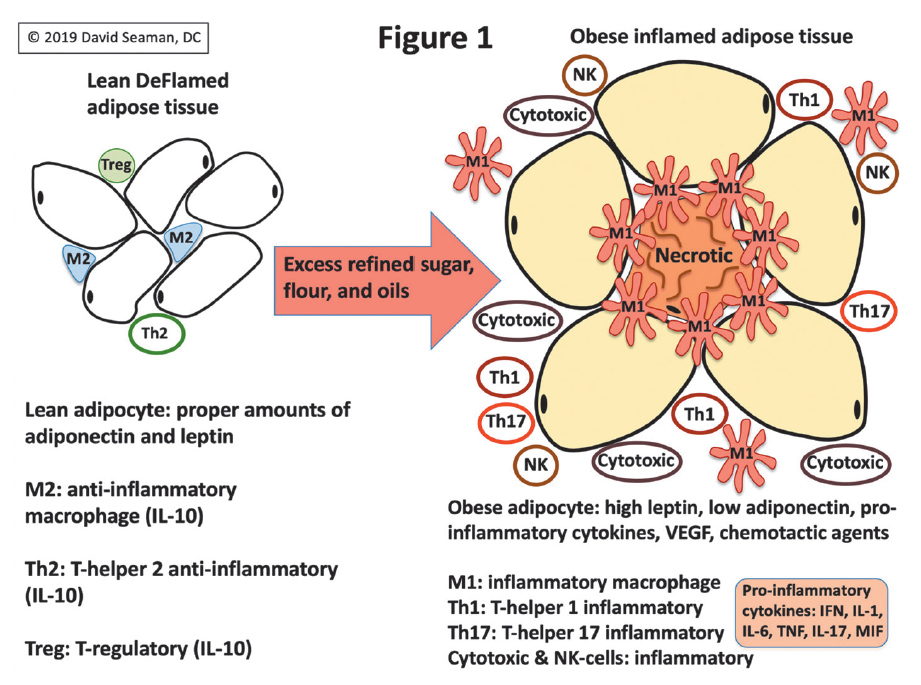
The immune cell profile in the pro-inflammatory state of obesity is very different compared to the lean state. Briefly, the cells that make up adipose tissue include adipocytes and immune cells. This was confirmed back in 2003, when it was realized that there was a pro-inflammatory shift in the macrophage population in obesity.5
Since that time, a great deal more research has outlined the immune cell changes that occur with obesity, such that there is also an accumulation of natural killer cells and cytotoxic T-cells. Interestingly, these immune cells otherwise do not accumulate unless one has a viral infection or cancer.
This means that the immune profiles of obese individuals are reflective of that of a viral infection state, as if the immune system is primed and ready to act. So, it is not surprising that obese people suffer more from acute respiratory infections than non-obese people:6
“Obese individuals are at an increased risk of outpatient visits for acute respiratory infection during both influenza and non-influenza season periods, suggesting that the effect of obesity on the risk of respiratory infections is not limited to influenza. Interventions designed to reduce the prevalence of obesity may have the added benefit reducing the population burden of respiratory infections.”
Considering the fact that human cells are vastly outnumbered by viruses, we are, in effect, already infected. And it should be viewed as a symbiotic infection and nothing to worry about until we develop the pro-inflammatory state of obesity and hyperglycemia. When this happens, there is an increased risk of having more frequent disruptions in virome homeostasis and the increased expression of viral infection symptoms.
I created Figure 1 for use in some of my books to illustrate the shift in the immune profile in lean versus obese adipose tissue. You should understand that the timeline involved in the transformation from a healthy immune profile to one that is overtly pro-inflammatory is variable.
In other words, obese people with the same body-mass index are not necessarily going to be equally pro-inflammatory, which is most readily assessed by testing for C-reactive protein, lipids, and glucose/A1c.
To be clear, I am not disputing that we can transmit infectious diseases; however, it does seem to me that most of our typical “infectious events” are disruptions in an individual’s personal homeostatic relationship with the 3 quadrillion viruses in their body, which leads to their proliferation and the resultant immune response that gives us infection symptoms.
And since we humans generally share a similar virome, the likelihood that our similar viromes could be particularly infectious to each other seems unlikely. Rather, it seems that we are more likely to spread novel viruses to each other, such as with COVID-19. We witnessed that such spread had minimal impact on healthy people, but was often catastrophic for obese individuals with hyperglycemia.
This would suggest that healthy people with a proper homeostatic relationship with their microbiome and virome are more readily able to adapt to a novel coronavirus that is otherwise of the same family of coronaviruses which occupy the human airway symbiotically. In other words, it may be that a pro-inflammatory obese and hyperglycemic body has lost the ability to effectively adapt.
With the above in mind, can you recall at any point during the COVID crisis when public health officials and/or politicians urged Americans to get to a healthy weight because one is much more likely to die from COVID and the flu if they are obese? How many urged Americans to get their vitamin D levels well into the normal range?
None made such recommendations and none urged Americans to take vitamin C and zinc, which will do no harm and likely help.1 These nutritional recommendations are essentially risk-free and can provide varying degrees of anti-inflammatory immune support depending on the individual.
It is really quite telling that “getting healthy” was never a message from public officials. And instead of losing weight and getting healthy, millions of Americans got fatter and sicker. Ironically, if you lived in New York City, Mayor de Blasio made a deal with Shake Shack to give you a free burger and fries as a reward for taking the jab.
So, it seems to me that people need to know that the human body contains about 30 trillion human cells, 39 trillion bacterial cells, and 3 quadrillion viruses; and that all three of these cell types can exist in homeostatic balance, so long as one avoids the pro-inflammatory state of obesity and hyperglycemia.
If we don’t, then we increase our risks of suffering a poor viral infection outcome, no matter the name of the virus. And by getting vitamin D levels into high normal range, and taking vitamin C and zinc, one is likely to get added protection.
Sadly, no health care profession truly rose up during COVID to promote health; how stunning this was to me. Certainly, it is not too late for acupuncture to take a leadership role in health promotion, since medicine has not.
This would actually be a very smart thing to do because America is more obese and hyperglycemic than before COVID emerged, which means Americans are even less prepared for the next novel virus, such that morbidity and mortality will be likely be much worse with the next one.
References
5. Seaman DR. The DeFlame Diet for Immune Health. Wilmington, NC: Shadow Panther Press, 2020.
6. Campitelli MA, Rosella LC, Kwong JC. The association between obesity and outpatient visits for acute respiratory infections in Ontario, Canada. Int J Obesity, 2014;38:113-119.
Mast cell activation syndrome (MCAS) affects more than 15% of the U.S. population but evades most practitioners’ radar. Just five years ago, it wasn’t even on my radar, despite already having 20 years of experience as a clinician at that time. The more I dug (similar to leaky gut and post-COVID syndrome), the more I found my patients were suffering from this disorder.
Research supports the effectiveness of selecting the distal acupuncture points for the treatment of microtrauma and for relieving pain, particularly in cases of chronic shoulder pain. But to make the treatment results long-lasting, clinical experience and research suggest that instead of treating the most painful structure first, we identify the inhibited driver, restore reliable recruitment, confirm it with immediate re-testing, and only then address the painful area as a branch of a deeper pattern.
The motivation behind our practice of medicine is important, impacting not just our experience but also the experiences of those we treat. It is perhaps for this reason that the aspiration to help not just some, but all beings heal, has historically been an important part of the medical tradition. To explain this, we need to consider how medicine is interwoven with other social domains.